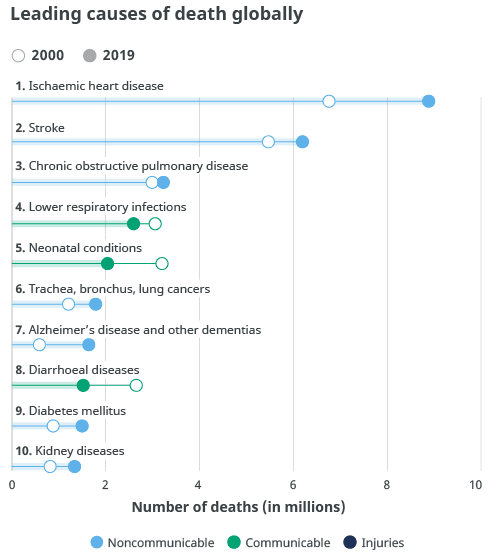
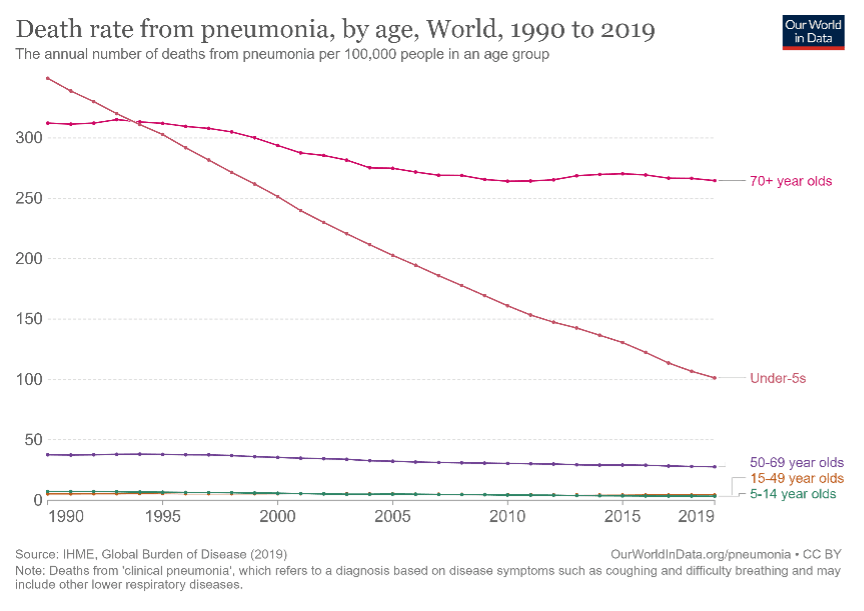
In countries classified as “low-income” by the World Bank, lower respiratory tract infections are the second most prevalent cause of death, while in “high-income” countries, they are the sixth-most common cause of death. Although the overall number of deaths from these infections has declined, pneumonia still caused 2.5 million deaths in 2019. The mortality rate among adults 70 and older remained largely the same over the past ten years (Pic. 2).
Historically, researchers considered bronchitis to have a primarily viral etiology and pneumonia to be primarily bacterial. Recent studies have provided more insights into the role of viral pathogens in pneumonia and the presence of bacterial and viral co-infections in patients with pneumonia, particularly in the pediatric population. One study estimated that 61% of cases of pneumonia requiring hospital admission in children younger than five years and without HIV infection had a primarily viral cause.1 Co-infections of respiratory viruses can also contribute to increased disease severity due to viral-viral and viral-bacterial interactions.2
Several presentations discussed community-acquired pneumonia (CAP), including determining risk factors, developing diagnostic methods, and managing severe CAP.
Even though the risk and predisposition factors for CAP development are well-known, researchers have paid much less attention to pre-existing nutrition status, which physicians typically consider when discussing disease management in oncology patients. M. Hegelund (Denmark) presented the results of an investigation comparing undernutrition and obesity with increased risk of death and the occurrence of new hospital admission after hospitalization with CAP.3
The prospective cohort study included 310 patients categorized as undernourished, well-nourished, and obese based on body mass index, age, weight loss, and fat-free mass index. Compared to well-nourished patients, undernourished patients had a higher risk of 30-day mortality, and obese patients had a higher risk of new hospital admission within 180 days. Neither undernutrition nor obesity was associated with a higher risk of in-hospital or 180-day mortality or new hospital admission within 30 days. Future studies should investigate the role of undernutrition and overnutrition in CAP-related outcomes to qualify therapeutic recommendations.
A. Liapikou (Greece) presented data from a large prospective study of adult patients hospitalized with clinically and radiographically confirmed CAP who were also tested for SARS-CoV-2.4 The study showed that patients who were SARS-CoV-2 positive had less severe pneumonia presentation but required more frequent mechanical ventilation (7.4% vs. 1.9%) and a longer hospital stay (mean 17.4 vs. 9.6 days). In-hospital mortality was similar between the two groups (7.9% in COVID-19 vs. 8.9% in non-COVID-19).
In another abstract, S. Mokaddem Mohsen (Tunisia) presented the results of a functional follow-up study of patients three months post-recovery from COVID-19 pneumonia.5 The results showed abnormal Carbon Monoxide Diffusing Capacity (DLCO), a surrogate marker of the available lung surface area. DLCO was decreased in 43% of patients. This decrease indicates a lessening gas exchange capability and, thus, worsening of respiratory function, which could be considered a marker of pulmonary vascular disease and predicts the potential development of pulmonary arterial hypertension.
Laboratory identification of the causative agent remains a major unmet need in pneumonia treatment and research. According to the current standards, a microbiological investigation should consist of at least a sputum culture, a blood culture, and a urinary antigen test for Streptococcus pneumoniae and Legionella pneumophila. Additional serologic tests for atypical bacterial pathogens may be performed but are not required.6 The etiology of CAP is identifiable in 53% to 75% of cases by the above criteria.7
The accuracy of rapid antigen and antibody detection tests in detecting the presence of CAP is high – 97-99% for all CAPs and 65-93% for Streptococcus pneumoniae. However, the ability to determine the exact etiology remains insufficient, with only 36-80% accuracy. For polymerase chain reaction (PCR) tests, the sensitivity is considerably higher at 58-98%, depending on the pathogen.
Before identifying a specific causative pathogen, the lack of rapid and accurate laboratory testing typically results in an initial empirical diagnosis. Misuse of antibiotics due to misdiagnosis is one of the causes of the development of resistant pathogens, now considered a “hidden pandemic.” From 2019 to 2020, there was an increase in drug-resistant infections of at least 15% for the following pathogens:8
B. Beovic (Slovenia) stressed that physicians must have reliable methods for an early diagnosis to administer an effective antibacterial treatment early.9 Rapid microbiology diagnostic methods have the potential to accelerate appropriate antibiotic treatment, but the results should be available at the bedside in real-time.
M. Sanguinetti (Italy) elaborated on the accuracy of rapid diagnostics for CAP in the emergency room.10 Physicians currently use several multiplex molecular platforms, including Unyvero, FilmArray, and FilmArray PN, to detect bacterial and non-bacterial pathogens that cause respiratory tract infections. Multiplex PCR tests accurately detect pathogens, but less than 50% of patients with pneumonia produce sputum, limiting these tests’ usefulness.11 The solution may be the application of nasopharyngeal swabs, which were used to test the FilmArray PN assay in patients admitted to the emergency room.12
A panel discussion chaired by A. Bush (UK) addressed the development of a new guideline for managing severe CAP.13 Physicians currently follow general guidelines covering both inpatient and outpatient settings and including all aspects of CAP management, with no specific additional treatment guidelines.14 However, patients with severe CAP – primarily defined as those admitted to the intensive care unit (ICU) – require a different treatment protocol. Even before the COVID-19 pandemic, the mortality rate among patients with severe CAP who developed acute respiratory distress syndrome (ARDS) or shock that required mechanical ventilation exceeded 30%. This trend led to the development of specific guidelines to address the needs of adult patients with severe CAP.
It is important to note that the new guideline’s definition of severe CAP excludes immunosuppression. The proposed protocol also does not include severity scores such as CURB-65 or the Pneumonia Severity Index (PSI) in the definitions. Panelist I. Martin-Loeches (Spain) stressed that only 35% of patients with a PSI risk class of 5 (the highest risk class requiring hospitalization) were admitted to the ICU.
He added that the new global protocols must also consider country-specific ICU admission criteria, as factors such as the availability and organization of ICUs and predominant regional pathogens will affect the choice of empirical antibiotic therapy. Experts from Europe and North and South America were involved in creating the global protocol; however, these guidelines will not encompass Asia.
Sun C. and Chen W. (Taiwan) compared the efficacy of Cefoperazone-sulbactam (CPZ-SBT) and piperacillin-tazobactam (PIP-TAZO) given as prolonged infusion for the treatment of severe pneumonia.15 Both antibiotics are known as effective treatments for pneumonia but are typically administered intramuscularly or intravenously twice daily for 7-21 days. The study compared the characteristics and outcomes of patients who received prolonged infusions of either CPZ-SBT or PIP-TAZO for more than five days for severe CAP, hospital-acquired pneumonia (HAP), or ventilator-associated pneumonia (VAP). The outcomes included clinical cure, effectiveness, and in-hospital mortality. The outcomes showed no differences between the two groups in treating pneumonia and proved the clinical efficacy of prolonged infusion.
RSV is one of the most common pathogens identified in adults with acute respiratory infections (ARI) and is increasingly recognized as a cause of illness in a high-risk adult population. Adults 65 and older with comorbid conditions such as human immune deficiency virus infection (HIV), congestive heart failure, COPD, or an immunocompromised status are considered “high risk.”
Treatment options for respiratory viral infections are limited to Oseltamivir, Zanamivir, and Peramivir for influenza, and there is no specific treatment currently available for RSV. Similarly, there are several approved and effective vaccines for influenza but none for RSV. Therefore, the treatment and prevention of RSV remain largely unmet medical need.
T. Shi (UK) investigated the disease burden of RSV-ARI in adults with comorbidities.17 She concluded that the incidence rate of RSV-ARI in patients 65 or older with comorbid conditions was much higher than in the general population (with or without comorbidities): 37.6 vs. 6.7 per 1000 persons per year. The hospitalization rate was also higher for those 65 and older than those 50–64 in both industrialized and developing countries. This data indicates that age might be an important risk factor for RSV-ARI–related hospital admissions among patients 50 and older. Similarly, RSV-ARI’s in-hospital case-fatality ratio (hCFR) was 11.7% for adults with comorbidity and 1.6% for the general population.
A. Langedijk (Netherlands) presented an alternative diagnostic approach for detecting RSV in children.18 Nasopharyngeal swabs are considered the gold standard for diagnosing RSV.
Although highly sensitive to the presence of RSV, they come with complications such as sample-acquiring burdens, time delays, and high personnel and resource costs. Moreover, the collection process can cause discomfort in the patient.
The authors evaluated the detection of RSV in paired nasopharyngeal and saliva samples with SalivaDirect+, a saliva-based PCR test authorized by the US FDA to detect SARS-CoV-2. Langedijk and team detected RSV in all saliva samples, which confirms that saliva may be a viable and preferable alternative to nasopharyngeal swabs for RSV detection. However, these results are preliminary due to the study’s main limitation – only 29 paired samples were taken, and only in infants, disregarding other age groups.